Antihistamine Driving Safety Checker
Input Your Details
How many hours ago did you take the pill?
Result
- Impairment Level:
- BAC Equivalent:
- Recommendation:
Select a medication and enter details to check your driving risk.
Imagine you are stuck in heavy traffic on a rainy Tuesday. Your eyes itch, your nose runs, and you reach for that familiar box of allergy pills in the glove compartment. You pop one, expecting relief, but what you get instead is a creeping sense of heaviness behind your eyelids. You tell yourself you are fine, but your reaction time just slowed down by seconds-seconds that could mean the difference between stopping safely and rear-ending the car ahead.
This scenario plays out every day for millions of drivers. Antihistamines are medications used to treat allergic reactions by blocking histamine receptors, but their impact on driving ability has been a major public safety concern since the 1980s. While we often think of alcohol as the primary danger on the roads, data shows that sedative H1 antihistamines are responsible for a significant portion of drug-related traffic deaths. Understanding which medications impair your driving-and knowing the legal consequences-is not just about avoiding a ticket; it is about staying alive.
The Three Generations of Antihistamines: Why Some Make You Drowsy
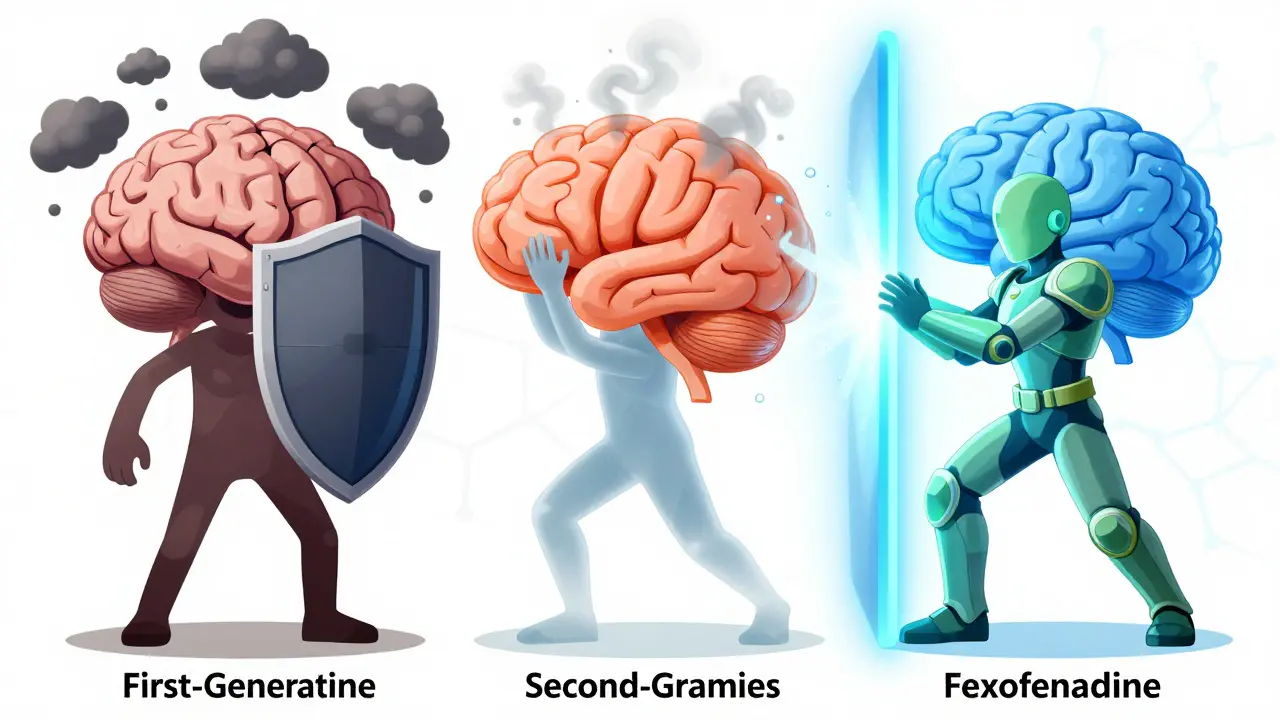
Not all allergy medications are created equal. To understand why some pills knock you out while others keep you alert, you need to look at how they interact with your brain. Doctors and researchers categorize antihistamines into three generations based on their chemical structure and how easily they cross the blood-brain barrier.
First-generation antihistamines include older drugs like diphenhydramine (Benadryl), triprolidine, and clemastine. These molecules are small enough to slip easily through the protective shield around your brain. Once inside, they bind to histamine receptors in the central nervous system, causing significant sedation. Think of them as blunt instruments-they stop the itch, but they also hit the brakes on your alertness.
Second-generation antihistamines, developed in the 1980s and 1990s, were designed to be smarter. Drugs like cetirizine (Zyrtec) and loratadine (Claritin) have larger molecular structures that make it harder for them to enter the brain. However, "harder" does not mean "impossible." Depending on your dose, body chemistry, and timing, these can still cause mild impairment. Cetirizine, for example, is known to cause drowsiness in about 15-20% of users, despite often being marketed as non-sedating.
Third-generation antihistamines represent the current gold standard for drivers. Medications like fexofenadine (Allegra) and levocetirizine (Xyzal) are engineered to stay largely outside the central nervous system. Clinical trials involving double-blind, placebo-controlled studies have shown that these drugs produce no statistically significant driving impairment after both single and repeated doses. If you drive regularly, these are the options you should prioritize.
| Generation | Common Examples | CNS Penetration | Driving Impairment Risk | Key Characteristic |
|---|---|---|---|---|
| First | Diphenhydramine, Clemastine | High | Severe (Equivalent to BAC 0.05-0.08%) | Causes significant sedation; long half-life |
| Second | Cetirizine, Loratadine | Moderate/Low | Mild to Moderate (Varies by individual) | Less sedating than first-gen, but cetirizine affects ~20% of users |
| Third | Fexofenadine, Levocetirizine | Minimal | Negligible/None | Safer for drivers; minimal CNS side effects |
How Much Do Antihistamines Actually Impair Your Driving?
You might feel fine, but your body tells a different story. Research from the U.S. National Highway Traffic Safety Administration (NHTSA) and independent psychopharmacologists reveals stark differences in performance depending on the medication.
First-generation antihistamines like diphenhydramine can increase lane deviation by 30-50% in standardized on-the-road tests. To put that in perspective, this level of impairment is equivalent to having a blood alcohol concentration (BAC) of 0.05-0.08%. In many jurisdictions, 0.08% is the legal limit for drunk driving. So, taking a common over-the-counter allergy pill can legally and physically put you in the same category as an intoxicated driver.
Second-generation drugs show more variable results. Loratadine generally shows minimal impairment in most studies. However, cetirizine at standard 10mg doses can cause a 15-20% increase in lane deviation. At higher doses, this impairment becomes significant. The danger here is subtlety. You may not feel "drunk," but your ability to react to sudden hazards-like a child running into the street or a braking car-is measurably slower.
Third-generation antihistamines, such as fexofenadine (180mg) and levocetirizine (5mg), demonstrate no statistically significant driving impairment compared to placebo in extensive testing. These drugs allow you to manage allergies without compromising your cognitive reflexes or motor skills.
The Hidden Danger: Tolerance and Additive Effects
A common misconception among regular users is that if you take the same medication every day, your body builds up a tolerance to the drowsiness. Dr. F. Estelle R. Simons, a leading expert in pediatrics and immunology, has reviewed this extensively. Her conclusion? While people report feeling less sleepy over time, objective tests show that clinical tolerance to the sedating effects is not consistently found. Your subjective feeling of alertness does not match your actual physiological impairment.
Even worse is the additive effect when combining antihistamines with other substances. If you mix first-generation antihistamines with alcohol, the impairment increases by 200-300% compared to either substance alone. This synergistic effect creates a dangerous cocktail that severely clouds judgment and slows reaction times. Even combining these drugs with other central nervous system depressants, like certain painkillers or anxiety medications, can amplify the risk significantly.
Another critical factor is the half-life of the drug. Diphenhydramine has a half-life of 4-12 hours. This means if you take it before bed, residual amounts can remain in your system the next morning, causing "hangover" drowsiness while you commute to work. Third-generation drugs offer an advantage here too, with half-lives of 11-14 hours but without the significant residual sedative effects because they do not penetrate the brain in the first place.
Legal Considerations: Is It Illegal to Drive on Antihistamines?
The laws surrounding medication and driving vary wildly depending on where you live, but the trend is moving toward stricter regulations. In the United States, there is no specific federal law prohibiting driving under the influence of prescription or over-the-counter medications unless you are impaired. However, if you are involved in an accident and toxicology reports reveal high levels of sedating antihistamines, you can be charged with reckless driving or DUI (Driving Under the Influence).
In Europe, the approach is more proactive. According to the European Medicines Agency, 22 countries have specific regulations prohibiting driving within 8-12 hours of using first-generation antihistamines. Fourteen countries classify certain sedating antihistamines as controlled substances requiring special driving permits. If you are traveling internationally, checking local laws is crucial. What is legal in your home country might land you in jail abroad.
Insurance companies are also catching up. The Insurance Institute for Highway Safety notes that widespread adoption of safer third-generation antihistamines could reduce medication-related crashes by 40-50% over the next decade. Conversely, failing to switch to safer alternatives when advised by a doctor could potentially impact insurance claims if negligence is proven.

Practical Safety Protocol: How to Drive Safely with Allergies
If you suffer from seasonal allergies or chronic rhinitis, you cannot simply avoid driving. Here is a practical checklist to ensure your safety and the safety of others:
- Switch to Third-Generation Meds: Ask your pharmacist or doctor about switching to fexofenadine or levocetirizine. These are widely available and specifically tested for driving safety.
- The 48-Hour Test Rule: Before you ever drive on a new antihistamine, take it at home for two days. Perform simple cognitive tasks, like reading or cooking, to gauge any subtle effects. Do not drive during this initial period.
- Timing Matters: If you must use a first-generation antihistamine (e.g., for severe acute symptoms), take it only at bedtime. Never take it before a planned drive.
- Read the Label: Over-the-counter products often bury driving warnings in small print. Look for phrases like "may cause drowsiness" or "do not operate machinery."
- Avoid Alcohol Completely: If you are taking any antihistamine, especially first or second-generation, do not consume alcohol. The combined effect is unpredictable and dangerous.
- Listen to Your Body: If you feel even slightly hazy, slow, or tired, pull over. As noted in Ford's Driving Skills for Life program, "feeling alert doesn't mean you're driving safely." Your self-assessment is likely flawed due to the medication's effects.
Cost vs. Safety: The Economic Reality
One barrier to switching to safer medications is cost. First-generation antihistamines like diphenhydramine are incredibly cheap, often averaging $4 per month. In contrast, third-generation options like fexofenadine can cost around $35 per month without insurance. This price difference leads some patients to stick with cheaper, riskier options.
However, consider the hidden costs. A single traffic violation, increased insurance premium, or minor accident can far exceed the annual savings of choosing a cheaper drug. Furthermore, generic versions of third-generation antihistamines are becoming more widely available, narrowing the price gap. Many employers and health systems now cover these safer alternatives precisely because they reduce workplace and road accidents.
The allergy medication market has shifted significantly, with fexofenadine capturing 38% of the U.S. antihistamine market by value in 2022. This shift reflects both consumer awareness and physician recommendations. Seventy-eight percent of physicians now prescribe third-generation antihistamines as first-line treatment for patients who drive.
Can I drive after taking Benadryl (diphenhydramine)?
It is strongly advised against. Diphenhydramine is a first-generation antihistamine that causes significant sedation and impairs driving skills to a degree similar to a blood alcohol content of 0.05-0.08%. It can also cause next-day drowsiness due to its long half-life. Wait at least 24 hours after your last dose before driving.
Is Zyrtec (cetirizine) safe for driving?
Zyrtec is a second-generation antihistamine and is safer than Benadryl, but it is not risk-free. Studies show that 15-20% of users experience measurable driving impairment, including increased lane deviation. If you choose to use Zyrtec, test it at home first and monitor your reaction times closely. For optimal safety, third-generation options like Allegra are preferred.
Which antihistamine is best for drivers?
Third-generation antihistamines, specifically fexofenadine (Allegra) and levocetirizine (Xyzal), are considered the safest for drivers. Extensive clinical trials have shown they produce no statistically significant driving impairment compared to a placebo, making them the top recommendation from medical authorities for anyone who operates a vehicle.
Does building tolerance to antihistamines make driving safer?
No. While you may subjectively feel less drowsy after taking the same medication repeatedly, objective tests show that physical impairment often remains. Your brain's perception of alertness does not align with your actual reaction time and motor control. Do not rely on tolerance as a safety measure.
What happens if I mix antihistamines with alcohol?
Mixing antihistamines, especially first-generation ones, with alcohol creates an additive effect that can increase impairment by 200-300%. This combination severely compromises judgment, coordination, and reaction time, drastically increasing the risk of a serious traffic accident. Avoid alcohol completely when taking these medications.